
From the 1Department of Orthopaedic Surgery and Musculoskeletal Medicine, University of Otago Christchurch, 2Burwood Academy of Independent Living, Burwood Hospital, Christchurch, New Zealand, 3Agency for Healthcare Research and Quality, Rockville, MD, 4Department of Rehabilitation Medicine, Georgetown University School of Medicine, and 5MedStar National Rehabilitation Hospital, Washington DC, USA
Objective: To examine associations between funding source, use of rehabilitation and outcomes after total joint replacement and to evaluate variations based on demographic characteristics.
Design: Cross-sectional, questionnaire-based national survey.
Subjects: Participants aged 45 years or older (n = 522) who received either private or public funding for their surgery, were recruited from the New Zealand Joint Registry 6 months after a total hip, total knee or unicompartmental knee replacement.
Results: The cohort was predominantly New Zealand European (90%), aged 68 years, with more men (55%) than women (45%). Privately funded participants were younger, had higher levels of education and employment, and lower rates of comorbidities at the time of surgery. Privately funded participants also reported spending less time on the surgical waiting list, were less likely to participate in pre-surgical rehabilitation, but reported more weeks of post-surgical rehabilitation and better patient-reported outcomes in terms of pain, function and quality of life, compared with their publicly funded counterparts.
Conclusion: Factors already known to impact on joint replacement outcomes were associated with funding source in this cohort. Socio-economic differences and inequities between private and public systems exist consistent with limited available prior research. In this cross-sectional study, no clinically significant differences in outcomes between the groups were identified. Prospective research will help to clarify whether funding source directly affects joint replacement rehabilitation outcomes.
Key words: total hip replacement; total knee replacement; rehabilitation.
Accepted Aug 30, 2019; Epub ahead of print Sep 10, 2019
J Rehabil Med 2019; 51: 00–00
Correspondence address: Deborah Snell, Department of Orthopaedic Surgery and Musculoskeletal Medicine, University of Otago Christchurch, New Zealand. E-mail: debbie.snell@otago.ac.nz
This study investigated whether the source of funding influences the use of rehabilitation services and patient outcomes after hip and knee replacement surgery. Patients who received either private insurance or public funding for their joint replacements were identified from a national joint register in New Zealand (n = 522) and invited to complete a survey 6 months after their operation. Study participants were mostly New Zealand European (90%), aged 68 years, with more men (55%) than women (45%). Privately-funded participants were younger, had more education, and were more likely to be employed than publicly-funded participants. Privately-funded participants also reported waiting less time for their operation, had more rehabilitation after their surgery, and reported better outcomes in terms of pain, function and quality of life, compared with their publicly-funded counterparts. There appear to be systematic differences between patients receiving public vs private insurance for joint replacement surgery, which raises concerns about unequal access to health services.
Joint replacement is an effective elective surgical intervention for degenerative joint disease, such as osteoarthritis (1–3). In New Zealand, as in other countries, the rates of primary hip and knee replacement are increasing (4, 5). Given the increasing prevalence of age-related joint disease, joint replacement demands are likely to continue to increase as the population ages and gains weight (3, 6). This, in turn, will increase the demand for associated health services, such as pre- and post-operative rehabilitation.
A number of factors have been described as drivers for the uptake of elective surgical procedures, such as total joint replacement (TJR). These include age, sex, ethnicity, and socioeconomic status (7, 8). Other related variables that may influence the use of such health interventions include education and health literacy, although these have been little studied (7). There is some evidence of inequities in the basis of surgery funding source (8), but little discussion regarding whether this funding source impacts the use of associated services, such as rehabilitation. In addition, research capturing drivers and outcomes of surgery and associated services funded in the private sector is limited (7). Use of rehabilitation services after TJR may also be impacted by other socio-economic barriers, including geography (9), where access to health services might depend on where a person lives and their employment status.
A recently published study evaluated equitable use of publicly funded hip and knee joint replacements in New Zealand (10). In this study the authors reviewed hospital discharge data for people undergoing TJR between 2006 and 2013, accessed from the Ministry of Health’s national minimal dataset. They reported that approximately 65% of TJRs were publicly funded for the period under study and that there was evidence of ethnic, socioeconomic and geographical inequity. For example, the authors reported that Māori and people in the most socioeconomically deprived groups had the highest rates of publicly funded TJR, possibly suggesting higher rates of privately funded procedures in other ethnic and socioeconomic groups. They also reported that those living in main urban centres had lower rates of publicly funded TJR. Again, the authors speculated that rates of privately funded TJR may be higher in larger urban centres. However, the use of associated services, such as rehabilitation, was not reviewed, and the authors did not have access to data from the private sector. This study raises questions regarding differences in the use of services and outcomes after TJR on the basis of funding source, and suggests that there may be inequities, particularly in terms of socioeconomic factors, ethnicity and geography.
Within New Zealand the majority of surgeons work in both public and private areas. Private surgery is funded by a “fee for service” arrangement with the funding agency, such as private insurance or the government-funded Accident Compensation Corporation (ACC), commonly by a “fixed price contract” for the whole procedure. Public hospitals either use salaried surgeons to perform the procedure, or outsource the procedure through a “fixed price contract”. Within the private area the great majority of surgeons work independently, with no ownership of the hospital facilities. Rehabilitation services are accessed either through the public hospital or independent private services, which are mostly owned and administered by physiotherapists. Often access to a private rehabilitation service is determined by whether the patient has funding, either from medical insurance or ACC.
Study objectives
The objectives of this study were to examine the associations between funding source (private vs public), use of rehabilitation, and outcomes before and after hip or knee replacement, and how these associations varied with education, socioeconomic status, geography and ethnicity.
Study design and recruitment strategy
The role of rehabilitation study is a cross-sectional questionnaire-based study characterizing rehabilitation therapy received before and during the first 6 months following primary total hip or knee, or unicompartmental knee replacement in New Zealand.
Participants were recruited from the New Zealand Joint Registry (NZJR) in order to achieve a national sample with geographical diversity. Because of the large numbers of registered primary hip and knee replacements, the NZJR obtains patient-reported outcome information from randomly selected patients across the country to achieve an annual response of 20% for each group (5). This was the sampling frame for the role of rehabilitation study. Flyers for the study were included in NZJR mail-outs between June 2015 and July 2016, and all patients returning flyers with their contact information were approached and invited to participate in the study.
The study received ethical approval from the University of Otago Human Ethics Committee (ref H14/070).
Participant selection
Patients registered and followed by the NZJR after elective primary hip or knee joint replacement in either private or public systems in New Zealand were eligible to participate in the study. The New Zealand health system is not dissimilar to that of other countries in the British Commonwealth. Selection criteria were broad and inclusive in order to capture patient variation and facilitate generalizability of findings. Thus, patients who met the following criteria were included in the study: (i) age 45 years or older, (ii) underwent primary unilateral total hip replacement (THR), total knee replacement (TKR), or unicompartmental knee replacement (UKR) for osteoarthritis 6 months prior to recruitment, (iii) agreed to participate in the study, and (iv) received either private or public funding for surgery. Patients with any previous operation on the index joint, those obtaining funding under New Zealand’s public accident and injury insurance scheme (ACC), and those who self-funded their surgeries, were excluded.
Data collection
Details were supplied monthly by the NZJR (name, preferred contact information) for potential participants meeting the inclusion criteria who had agreed to being contacted by the study team. Potential participants were then contacted by a research assistant to discuss the study and invite participation.
Once recruited, role of rehabilitation participants completed questions in booklet form regarding timing, type, intensity and duration of any rehabilitation following referral for joint replacement (pre- and post-operatively). Demographic and clinical questions were also included (date of birth, ethnicity, geographical location (region and population size), funder (public funding vs private funding), medical history). A final text box was available for any additional comments participants wished to add. Questionnaires were available for completion either online (e.g. Survey Monkey™) or by post, depending on the participant’s preference.
Additional clinical information was collected from the NZJR. This included pain and functional outcomes at 6 months post-operation using Oxford scores (11, 12), procedure type, date of surgery, body mass index, and an indication of comorbidity burden at time of surgery using the American Society of Anaesthesiologists (ASA) classification (13). Access to this clinical information minimized participant burden by avoiding duplication of data collection from participants.
Study variables
Demographic variables included age, sex, ethnicity, highest education level, work status, funder of surgery (public, private). Clinical and surgical variables included pre-existing medical conditions/comorbidities (self-reported and ASA classification); body mass index, procedure type (THR, TKR, UKR), and time on the surgical waiting list (weeks). Rehabilitation variables included time from surgery to first rehabilitation session (weeks); pre- and post-operative rehabilitation type (physiotherapy, occupational therapy, other), setting (home-based programme, outpatient clinic-based rehabilitation, other), frequency/intensity (times per week, number of weeks/mean duration of sessions); and number of outpatient follow-up reviews with the surgeon. Six-month self-reported post-operative outcomes were collected as follows: pain and function outcomes with the Oxford Hip and Knee Scores (11, 12); quality of life with World Health Organization Quality of Life 8-item questionnaire (WHOQOL-8 (14, 15)).
Data analyses
First, the sample was characterized by funding source in terms of demographic status, health status (e.g. presence of comorbidities, body mass index), procedure type, geographical location, participation in any pre- and/or post-operative rehabilitation and outcomes using descriptive statistics. Secondly, for those who obtained rehabilitation services before and/or after their operation, the setting (e.g. home-based programme, outpatient clinic, other), time from surgery to first rehabilitation session, the duration, intensity (times per week/total hours), and how rehabilitation services and practice patterns varied based on funding source and geography were identified. Bivariate analyses then tested relationships between funding source, demographic, clinical and rehabilitation variables. Contingency tables (cross-tabs) were calculated for discrete variables and χ2 tests determined significance of 2-way associations. For continuous variables, independent-samples t-tests, or analysis of variance were used. Results are reported as odds ratios or mean differences, and 95% confidence intervals (95% CI).
List-wise deletion, the default SPSS approach to account for missing data, was used. This was considered appropriate due to sample size and the limited amount of missing data (< 3%) across variables.
A total of 768 people who met the role of rehabilitation study inclusion criteria agreed to contact from the study team and returned flyers to the NZJR with their preferred contact information. Of these, 608 were successfully recruited into the study and returned questionnaires (79.2% response rate; n = 158 online and n = 450 by post). Of those who agreed to initial contact, but who were not recruited into the study, 17 subsequently declined to participate (too ill, moved away, changed their mind) or were deceased at time of contact (n = 1). Of the remaining patients, 54 were contacted and agreed to participate, but did not return their questionnaires after 3 reminders and 88 could not be contacted. No data were available in this study regarding non-recruited participants to determine if there were any differences in response rate on the basis of funding source. A small number of recruited participants reported that they received funding from ACC (n = 56) or self-funded their surgery (n = 28) and were not included in analyses. Thus, of the full recruited cohort, n = 522 represented the sample included in analyses for the current study.
Description of study sample
A summary of participant demographic and clinical characteristics is provided in Table I. The mean age of participants was 67.8 years (SD 8.7, range 44–89 years). There were slightly fewer women (45.0%) than men (55.0%); the sample was predominantly New Zealand European (90.0%); 70.5% reported high-school or tertiary level qualifications and 43% of participants were in either full- or part-time employment at the time of surgery.
Table I. Demographic and clinical characteristics of the study sample on the basis of funding type (n = 522)
When demographic and clinical variables were examined by funding source, the analyses indicated participants privately funded were, on average, younger than publicly funded participants (mean difference (MD) = 4.4, 95% CI 2.9–5.9, p < 0.01) and had higher levels of education (high-school or tertiary qualifications: χ2 (3) = 18.8, odds ratio (OR) 1.6, 95% CI 1.2–2.1, p < 0.01). They were also more likely to be in either full- or part-time employment (χ2 (3) = 37.6, OR (in employment) 1.8, 95% CI 1.5–2.2, p < 0.01). Those with private funding had lower levels of comorbidity (χ2 (3) = 16.5, OR (ASA score 1) 1.4, 95% CI 1.1–1.8, p < 0.01), spent less time on a surgical wait-list (MD = 42.9 weeks, 95% CI 36.1–49.7, p < 0.01) and demonstrated better outcomes in terms of reduced pain and improved function and quality of life, compared with publicly funded participants (total Oxford score: MD = 2.0, 95% CI 0.7–3.3, p < 0.01; WHOQOL-8 total score: MD = 1.9, 95% CI 1.1–2.8, p < 0.01). There were no other significant differences between the 2 groups. These results are also shown in Table I.
Extent of rehabilitation (intensity, duration, type) and funding source
Table II shows the breakdown of pre- and post-operative rehabilitation on the basis of funding source. These analyses indicate that privately funded participants were less likely to participate in rehabilitation before surgery than publicly funded participants (χ2 (1) = 11.3, OR 1.5, 95% CI 1.2–2.0, p < 0.01), but there were no differences in use of rehabilitation between the groups following surgery. However, privately funded participants participated in more weeks of rehabilitation post-operatively (weeks of post-operative rehabilitation: MD = 1.8, 95% CI 0.4–3.2, p < 0.05), and had more post-operative surgical follow-up (post-operative surgical reviews: MD = 0.5, 95% CI 0.3–0.7, p < 0.01)
Table II. Pre- and post-rehabilitation characteristics by funding type (n = 522)
There were no significant differences in terms of funding or use of rehabilitation on the basis of ethnicity. However, almost 90% of the sample was of New Zealand European ethnicity, with New Zealand Māori making up just 5.0%. The low numbers of non-New Zealand European participants prevented meaningful evaluation of associations (see Table I). As shown in Table I, there were no significant differences on the basis of geography and those receiving private or public funding for surgery for the sample as a whole, although there were differences when groups were examined separately on the basis of the joint replaced (see below and Tables III–V).
Total hip replacement. Table III shows the breakdown of demographic, clinical and rehabilitation characteristics for participants with THR (n = 189). Privately funded THR participants were younger than their publicly funded counterparts (MD = 5.4, 95% CI 2.6–8.2, p < 0.01), and were more likely to be working (χ2 (1) = 24.1, OR 2.6, 95% CI 1.7–3.9, p < 0.01). They spent less time on the surgical waiting list (MD = 36.8 weeks, 95% CI 28.8–44.7, p < 0.01), and reported less pain, improved function and quality of life outcomes at 6-months after surgery (total Oxford: MD = 2.2, 95% CI 0.2–4.2, p < 0.05; WHOQOL-8: MD = 2.2, 95% CI 0.8–3.7, p < 0.01). In terms of use of rehabilitation, privately funded participants were less likely to have used rehabilitation before surgery (χ2 (1) = 5.6, OR 1.7, 95% CI 1.1–2.7, p < 0.01), but were just as likely to have participated in rehabilitation after surgery as publicly funded participants. There were no other differences between the groups.
Table III. Demographic, clinical and rehabilitation characteristics of participants with total hip replacement on the basis of funding type (n = 189)
Total knee replacement. Table IV shows the breakdown of demographic, clinical and rehabilitation characteristics for participants with TKR (n = 273). Privately funded TKR participants were younger than their publicly funded counterparts (MD 3.8, 95% CI 2.0–5.7, p < 0.01); had higher levels of education (χ2 (1) = 10.6, OR 1.8, 95% CI 1.2–2.79, p < 0.01); were more likely to be working (χ2 (1) = 6.7, OR 1.4, 95% CI 1.1–1.9, p < 0.05); and more likely to be living in an urban area (χ2 (1) = 17.6, OR 0.6, 95% CI 0.4–0.7, p < 0.01). They spent less time on the surgical waiting list (MD = 45.1 weeks, 95% CI 33.9–56.2, p < 0.01) and self-reported higher quality of life outcomes 6 months after surgery than their publicly funded counterparts (WHOQOL-8: MD = 1.5, 95% CI 0.3–2.7, p < 0.05). In terms of use of rehabilitation, privately funded participants were less likely to have used rehabilitation after surgery (χ2 (1) = 4.1, OR 1.5, 95% CI 1.1–2.1, p < 0.05) and reported more reviews with their surgeon post-operatively than publicly funded participants (MD = 0.5, 95% CI 0.3–0.8, p < 0.01). However, privately funded participants who did use post-operative rehabilitation, participated in more weeks of rehabilitation than publicly funded participants (MD = 3.0, 95% CI 1.2–4.9, p < 0.01). There were no other differences between the groups.
Table IV. Demographic, clinical and rehabilitation characteristics of participants with total knee replacement on the basis of funding type (n = 273)
Unicompartmental knee replacement
Table V shows the breakdown of demographic, clinical and rehabilitation characteristics for participants with UKR (n = 60). Privately funded UKR participants were younger than their publicly funded counterparts (MD 4.3, 95% CI 0.0–8.7, p = 0.05); and were more likely to be working (χ2 (1) = 4.7, OR 1.9, 95% CI 1.0–3.6, p < 0.05). They spent less time on the surgical waiting list (MD = 57.6 weeks, 95% CI 36.4–78.7, p < 0.01) and self-reported higher quality of life outcomes 6 months after surgery (WHOQOL-8: MD = 3.0, 95% CI 0.6–5.4, p < 0.05). In terms of use of rehabilitation, although the numbers are small, privately funded participants were less likely to have used rehabilitation before surgery, but were just as likely to have participated in rehabilitation after surgery as publicly funded participants. Privately funded participants also reported more follow-up visits with their surgeon post-operatively than their publicly funded counterparts (MD = 0.7, 95% CI 0.0–1.4, p = 0.05). There were no other differences between the groups.
Table V. Demographic, clinical and rehabilitation characteristics of participants with unicompartmental knee replacement on the basis of funding type (n = 60)
This study examined associations between funding source (private vs public), use of rehabilitation and outcomes before and after hip or knee replacement, and how these associations varied with education, socioeconomic status, geography and ethnicity. Although there was some variation based on the joint replaced, a pattern of differences based on surgery funding source was evident. It was found that participants who had surgery funded in the private sector were more likely to be younger, have higher levels of education, be employed, and have lower rates of comorbidities at the time of surgery. These participants also reported spending less time on the surgical waiting list and were less likely to participate in pre-surgical rehabilitation. Privately funded participants using rehabilitation following surgery reported more weeks of rehabilitation and better patient-reported outcomes in terms of pain, function and quality of life, compared with their publicly funded counterparts. No significant differences in terms of geography and funding source were identified, although those with private funding undergoing TKR seemed more likely to live in an urban area. It was not possible to examine impacts of funding source and outcomes by ethnicity because of the small numbers of non-European participants in the study sample.
The findings of this study may reflect policy differences between public and private funding systems for elective surgeries. While less use of pre-surgical rehabilitation may simply reflect faster progression to surgery from assessment by the surgeon for privately funded participants, the findings that privately funded participants accessed rehabilitation for longer after surgery is interesting. This might reflect policy and systemic differences based on resourcing. Pressures in the public system may mean that rehabilitation goals and length of stay in rehabilitation are resource-driven rather than person-driven. Anecdotally, publicly funded physiotherapy interventions tend to focus on short-term functional outcomes, such as reduced reliance on walking aids. Private physiotherapy, on the other hand, may have the flexibility to set more individualized activity and participation goals, including return to exercise, sport and employment. Some of the free-text comments that participants added to their questionnaires reflect these differences and also express dissatisfaction with rehabilitation available through the public system. For example, one participant who was funded in the public system wrote:
“The initial 12 sessions doing exercises at the hospital gym were fine, but only get you through those 5 weeks or so. It takes months to build up your muscles after a hip replacement. My thigh muscles had disappeared. If all I wanted was to be able to walk to the letter box and make the bed, fine, but I wanted to do weekend tramps, walk to work, cycle, sail, etc.”
Another participant expressed feelings of abandonment and anxiety linked to limited rehabilitation support in the public system:
“The initial rehab did help, but now I’ve just got to keep doing the exercises and have had no back up from physio to see my progress … Sometimes I feel I’ve been abandoned and left to get on with it by myself.”
A key focus of the present study was to examine whether surgical funding source made a difference in terms of outcomes and use of rehabilitation. All participants, on average, reported good clinical outcomes in terms of reduced pain and improved function and quality of life. Privately funded patients had better 6-month outcomes in terms of pain, function, and quality of life, which were statistically significant, but perhaps not clinically relevant. There was a difference of only 2 points on the Oxford and WHOQOL-8 questionnaires, respectively (16). Moreover, in the absence of pre-surgical data, it is difficult to determine if these findings truly reflect better outcomes for the privately funded group. Privately funded participants were younger, had fewer comorbidities, and spent less time waiting for their surgery. It is possible that privately funded participants had less pain, higher function and quality of life before their surgery than did publicly funded participants. Without being able to evaluate change before and after surgery, it is difficult to determine if funding source was indeed associated with outcomes in this study or whether other factors, such as wait time for surgery, better explain outcomes. Future research is needed to consider the effects of a patient’s pre-surgical status.
While outcomes on the basis of funding source were difficult to evaluate directly, variables known to impact outcomes did appear to be associated with funding source. For example, privately funded participants reported spending less time on the surgical waiting list and had faster access to surgical intervention. We have shown previously that wait list times contribute to outcomes following THR and TKR (Snell, D. Personal communication, Sep 12, 2019). There is also growing evidence supporting the effects of psychological factors on joint replacement outcomes, such as illness beliefs and expectations, locus of control and self-efficacy. Accessing surgery without a long wait and having economic resources to do so may enhance self-efficacy, satisfaction with joint replacement and outcomes (17, 18). For example, free-text comments from participants reflected the importance of timely access to surgery:
“I think the replacement operation can happen too late for some people. Pain and not being able to do things get people down and the recuperation takes longer; I didn’t want to have to wait until I couldn’t move to have the operation.”
The findings of the current study also resonate with previous research considering equity of access to joint replacement surgery. For example, in the systematic review by Mújica Mota and colleagues (8), socio-economic circumstances, such as being in paid employment and having health insurance, impacted on surgery uptake, and higher levels of education were associated with motivation to seek timely surgical interventions. Prior studies evaluating equitable access to joint replacement surgery in the UK (7) and New Zealand (10) suggested there were geographical differences, with those in urban centres having lower rates of publicly funded joint replacement. This suggests there are relationships between socio-economic and geographical factors, although these studies did not conduct comparisons between privately and publicly funded cases. However, the current study did not find systematic differences in rates of joint replacement or use of rehabilitation services on the basis of geographical location.
Study limitations
This study has several limitations. One limitation is the representativeness of the study participants. While the study captured geographical diversity, study participation was voluntary and thus presents potential for selection bias. It was not possible to analyse differences between responders and non-responders to determine the extent of such bias. As noted, the NZJR captures more than 95% of joint replacements in New Zealand, but only samples 20% of this larger group for follow-up collection of patient-reported outcome data (5). An even smaller proportion of this 20% was sampled, taking into account NZJR response rates. However, when we considered the demographic and clinical features of the wider NZJR population, role of rehabilitation sample appears very similar in terms of variables, such as age, sex, comorbidity burden and procedure type.
It is also possible that our sampling method and frame resulted in systematic bias regarding those participating in our study, under-representing the experiences of certain subsections of our target population. Important subgroups within New Zealand’s population, such as Māori, may not have been captured. Participants responding to our survey were predominantly New Zealand European and rates across ethnicity categories were inconsistent with general New Zealand population statistics (4, 19), and other studies examining rates of TJR among Māori and non-Māori (20). We can only speculate on the reasons for lack of ethnic diversity in our sample. It has been well demonstrated that Māori have the poorest health status of any ethnic group in New Zealand (20), although there is limited evidence to suggest lower rates of TJR among Māori compared with non-Māori in publicly funded systems in New Zealand (4, 10). There is, however, good evidence to suggest that Māori may be difficult to reach in terms of participation in health research and intentional strategies are required by researchers achieve recruitment equity (21, 22).
There is a possibility that referral bias underpins, to some extent, differences in rehabilitation between groups. For example, some surgeons may have been more likely to have referred patients to rehabilitation than others. This study did not capture particular surgeons operating on participants, and so any such patterns or potential for bias were not examinable. In addition, our study is not able to shed light on the impacts of incentives/disincentives in either public or private systems, or optimal levels of rehabilitation to determine whether the public system under-provides or the private system over-provides rehabilitation services. These are issues that should be a focus of future studies.
Finally, we asked participants to recall details regarding access to rehabilitation extending back many months and the reliability of the survey itself has not been examined. This raises a concern about the accuracy of data collection as a result of recall bias. This may be reflected in variability evident in the self-reported data, most notably with regard to pre-surgical variables. None-theless, this analysis drew on the experiences of more than 500 participants, which makes this study one of the larger published studies seeking to characterize access to rehabilitation before and after joint replacement.
Conclusion
This study investigated whether the source of funding for surgery (private vs public funding) was associated with use of rehabilitation and outcomes following hip and knee joint replacements. The findings suggest that factors already known to affect health outcomes, such as length of time on a surgical waiting list, satisfaction with rehabilitation, and self-efficacy, were associated with funding source. Those with private funding for their joint replacements and associated rehabilitation also tended to be younger, have higher levels of education, be in employment, and have fewer comorbidities, than their publicly-funded counterparts. These findings suggest that socio-economic differences and inequities based on funding source exist and are consistent with prior research, although previous research is limited. Clinically significant differences in pain and function outcomes between the groups based on funding source were not identified in this sample. Prospective randomized trials that examine pain and functional outcomes will help to clarify whether funding source directly impacts on outcomes.
The authors would like to thank research assistant Caroline Norris for her assistance with recruitment and data collection. We acknowledge and thank the staff at the New Zealand Joint Registry who assisted with recruitment and provision of additional data. We also acknowledge the Burwood Academy of Independent Living (BAIL) for hosting the research grant.
Funding. This research was supported by a Project Grant from the Canterbury Medical Research Foundation (Grant no 14/07).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize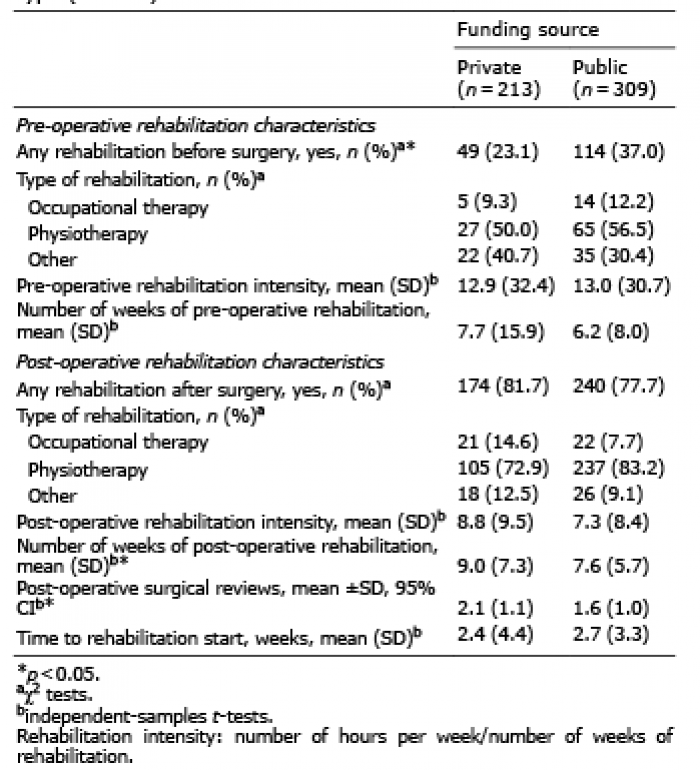 Click to show fullsize
Click to show fullsize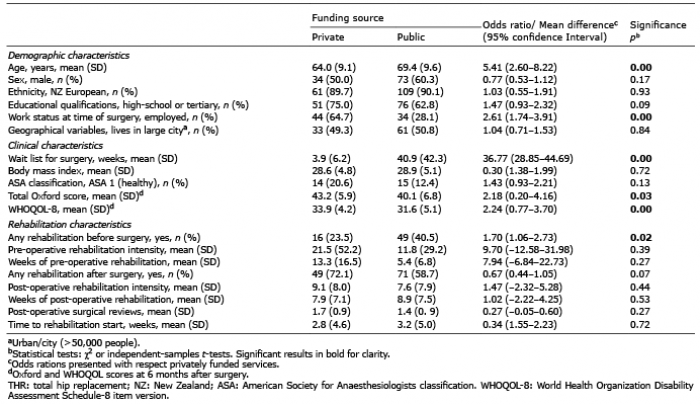 Click to show fullsize
Click to show fullsize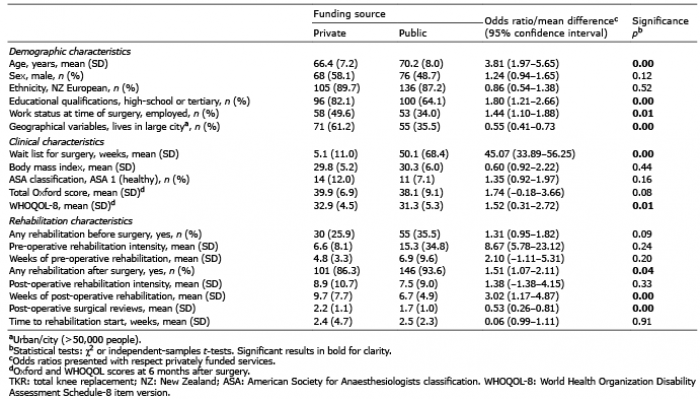 Click to show fullsize
Click to show fullsize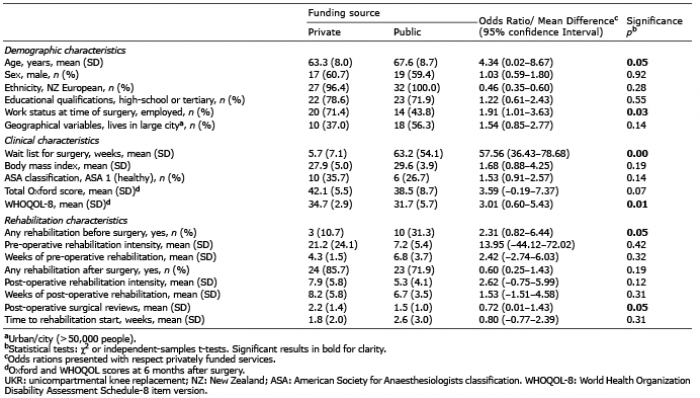 Click to show fullsize
Click to show fullsize